
Cocaine related oronasal fistula (hole) real life case
Cocaine: a powerfully addictive stimulant drug
made from the leaves of the coca plant native to South America
Nowadays, patients who use cocaine, come to realize the effects it has on their nose and palate as it destroys it. Unfortunately, they are not keen to admit or discuss cocaine consumption or deny their addiction, or even the duration of cocaine sniffing.
They come to our practice for immediate help and assistance, that is why we always rule out other conditions that can cause similar situations such as infections, neoplasms, systemic diseases (granulomatosis), or even exposure to other chemicals since we do thorough investigation and background check of the patient.
We are not here to judge the patient, we are here to help the patient become aware of the damage that occurred because of cocaine use, and how we can fix the problem. Of course, the first thing we advise the patient before any steps of treatment begin, is to abstain from using cocaine.
The question that arises though is this: Is patient ready to abstain? Shall he ask for help from other professionals as well? What are the symptoms of such a situation?
In short, the symptoms of oronasal fistula are as below:
- Rhinolalia (nasal quality of speech)
- Regurgitation of food and liquids in the nose when swallowing
- Anosmia
- Halitosis(cacosmia)
- Pain
- Headache
- Epistaxis
Bearing in mind the above symptoms, we proceed in clinical examination, which usually leads us to the following findings:
- Nasal septal perforation
- Diffuse necrotizing ulcerative lesions
- Saddle nose
- External cutaneous ulcers of the nose
- Lateral nasal wall destruction
- Hard and soft palate perforation
When cocaine use becomes chronic then we observe CIMDL (cocaine induced midline destructive lesions) which means that we have wider osteocartilaginous destruction of nose, sinus, palate, thus we need a CT scan for bone destruction and an MRI with contrast for nasal /paranasal mucosa and soft tissue erosion
In order to proceed in Lab Tests, we shall need from the patient:
- Urine sample (up to 3 days)
- Blood sample (up to 2 days)
- Hair sample (months to years)
In order to proceed in the Treatment, the patient must have an adequate period of abstinence of at least 6 months which usually is a challenge. Continued abstinence, in fact, is an absolute requirement that patients must fulfil to consider surgical reconstruction. Early treatment choice at the beginning of abstinence allows for the Palatal obturator to be added.
The medical therapy consists of regular saline cleaning of the area, careful debridement of necrotic tissues and crusts, administration of systemic or topic antibiotic therapy.
Early treatment choice at the beginning of abstinence allows for the Palatal obturator to be added.
In the case of Surgical Intervention, the use of the following is required:
- Local flaps i.e palatal /lingual flaps: ischemic tissues-may cause more necrosis
- Regional flap: temporalis pedicled flap, submental island flap
- Free vascularized tissue: ALT, Radial forearm free flaps
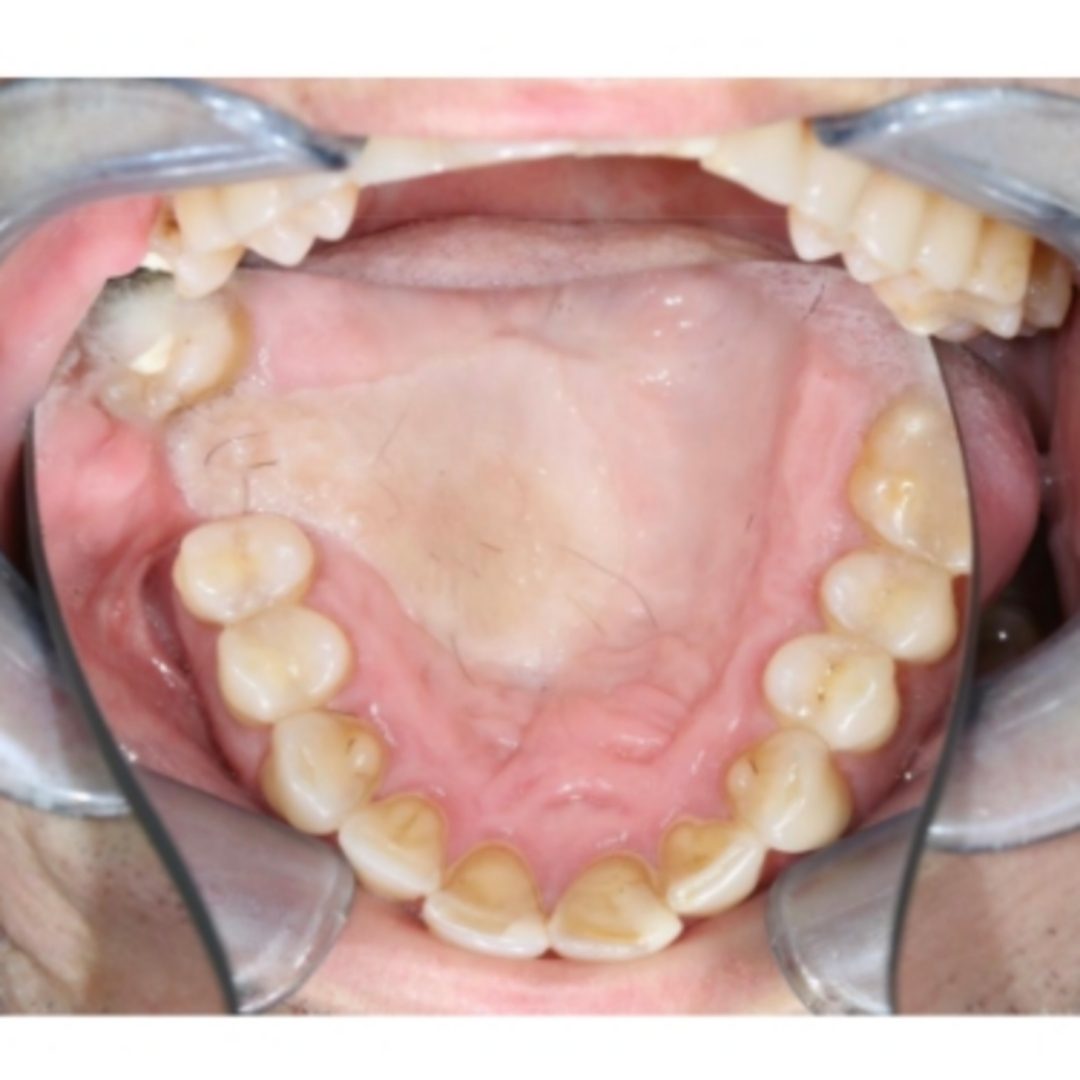
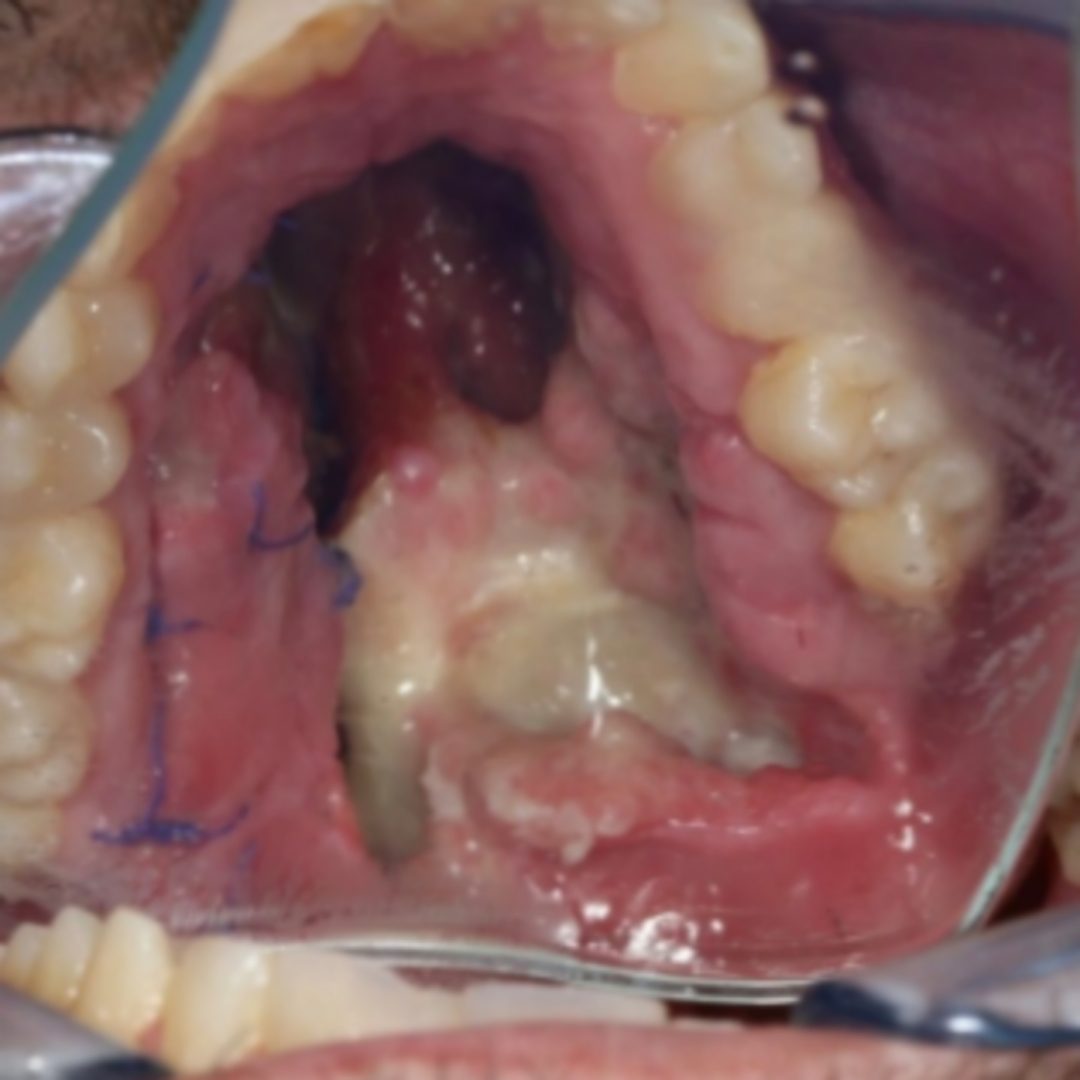
Real Patient Case of 34-Year-old Male:
Our patient, a 34-year-old man with a 10-year history of intranasal abuse of cocaine which led to hard palate perforation. He had 2 previous surgeries with local flaps, but osteomyelitis was diagnosed. Culture taken and treated accordingly with antibiotics for 6 months prior to surgery. The patient was complaining about regurgitation of food and liquids in the nose. Of course, we referred him to a habilitation center in which he went for 4 months and after another 8 months of abstinence (we checked with consecutive urine analysis) we agreed on the date for the surgery.
We proceeded with the surgical intervention by using the radial Fascio cutaneous forearm free flap. We performed the Allen Test to check collateral circulation from ulnar artery while we did the relevant preoperative drawing of the flap on the forearm, to mark the area of skin we would need and use.
The surgery was crowned with great success and the patient is cocaine free-long term thus the stable result. It is of the essence to mention that the radial free flap is the only way to treat cocaine related oronasal fistula cases but we have to point out that there can be a flap failure if the patient does not comply with cocaine long term abstinence.